

Male hypogonadism
![]() January, 3rd, 2025
January, 3rd, 2025
Benefit Summary
This condition affects the ability of men’s bodies to produce enough testosterone or enough sperm or both.
Overview
, Overview, ,
Male hypogonadism is a condition in which the body doesn’t produce enough of the hormone that plays a key role in masculine growth and development during puberty (testosterone) or enough sperm or both.
You can be born with male hypogonadism, or it can develop later in life, often from injury or infection. The effects — and what you can do about them — depend on the cause and at what point in your life male hypogonadism occurs. Some types of male hypogonadism can be treated with testosterone replacement therapy.
Symptoms
Hypogonadism can begin during fetal development, before puberty or during adulthood. Signs and symptoms depend on when the condition develops.
Fetal development
If the body doesn’t produce enough testosterone during fetal development, the result may be impaired growth of the external sex organs. Depending on when hypogonadism develops and how much testosterone is present, a child who is genetically male may be born with:
- Female genitals
- Genitals that are neither clearly male nor clearly female (ambiguous genitals)
- Underdeveloped male genitals
Puberty
Male hypogonadism can delay puberty or cause incomplete or lack of normal development. It can hamper:
- Development of muscle mass
- Voice deepening
- Growth of body and facial hair
- Growth of the penis and testicles
And it can cause:
- Excessive growth of the arms and legs in relation to the trunk of the body
- Development of breast tissue (gynecomastia)
Adulthood
In adult males, hypogonadism can alter certain masculine physical characteristics and impair normal reproductive function. Early signs and symptoms might include:
- Decreased sex drive
- Decreased energy
- Depression
Over time, men with hypogonadism can develop:
- Erectile dysfunction
- Infertility
- Decrease in hair growth on the face and body
- Decrease in muscle mass
- Development of breast tissue (gynecomastia)
- Loss of bone mass (osteoporosis)
Severe hypogonadism can also cause mental and emotional changes. As testosterone decreases, some men have symptoms similar to those of menopause in women. These can include:
- Difficulty concentrating
- Hot flashes
When to seek help
See your health care provider if you have symptoms of male hypogonadism. Finding the cause of hypogonadism is an important first step to getting appropriate treatment.
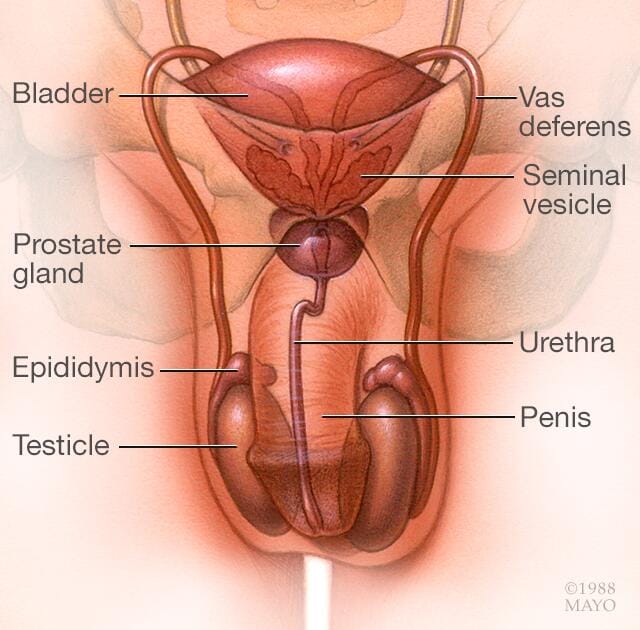
Male hypogonadism means the testicles don’t produce enough of the male sex hormone testosterone. There are two basic types of hypogonadism:
- Primary. This type of hypogonadism — also known as primary testicular failure — originates from a problem in the testicles.
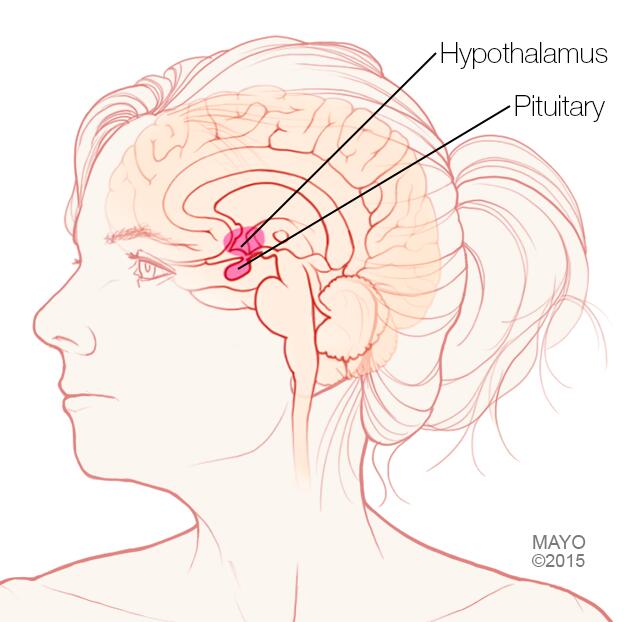
- Secondary. This type of hypogonadism indicates a problem in the hypothalamus or the pituitary gland — parts of the brain that signal the testicles to produce testosterone. The hypothalamus produces gonadotropin-releasing hormone, which signals the pituitary gland to make follicle-stimulating hormone (follicle-stimulating hormone (FSH)) and luteinizing hormone (luteinizing hormone (LH)). Luteinizing hormone then signals the testes to produce testosterone.
Either type of hypogonadism can be caused by an inherited (congenital) trait or something that happens later in life (acquired), such as an injury or an infection. At times, primary and secondary hypogonadism occur together.
Primary hypogonadism
Common causes of primary hypogonadism include:
-
Klinefelter syndrome. This condition results from a congenital abnormality of the sex chromosomes, X and Y. A male normally has one X and one Y chromosome. In Klinefelter syndrome, two or more X chromosomes are present in addition to one Y chromosome.
The Y chromosome contains the genetic material that determines the sex of a child and related development. The extra X chromosome that occurs in Klinefelter syndrome causes abnormal development of the testicles, which in turn results in underproduction of testosterone.
-
Undescended testicles. Before birth, the testicles develop inside the abdomen and normally move down into their permanent place in the scrotum. Sometimes one or both of the testicles aren’t descended at birth.
This condition often corrects itself within the first few years of life without treatment. If not corrected in early childhood, it can lead to malfunction of the testicles and reduced production of testosterone.
- Mumps orchitis. A mumps infection involving the testicles that occurs during adolescence or adulthood can damage the testicles, affecting the function of the testicles and testosterone production.
- Hemochromatosis. Too much iron in the blood can cause testicular failure or pituitary gland dysfunction, affecting testosterone production.
- Injury to the testicles. Because they’re outside the abdomen, the testicles are prone to injury. Damage to both testicles can cause hypogonadism. Damage to one testicle might not impair total testosterone production.
-
Cancer treatment. Chemotherapy or radiation therapy for the treatment of cancer can interfere with testosterone and sperm production. The effects of both treatments often are temporary, but permanent infertility may occur.
Although many men regain their fertility within a few months after treatment, preserving sperm before starting cancer therapy is an option for men.
Secondary hypogonadism
In secondary hypogonadism, the testicles are normal but don’t function properly due to a problem with the pituitary or hypothalamus. A number of conditions can cause secondary hypogonadism, including:
- Kallmann’s syndrome. This is an abnormal development of the area of the brain that controls the secretion of pituitary hormones (hypothalamus). This abnormality can also affect the ability to smell (anosmia) and cause red-green color blindness.
-
Pituitary disorders. An abnormality in the pituitary gland can impair the release of hormones from the pituitary gland to the testicles, affecting normal testosterone production. A pituitary tumor or other type of brain tumor located near the pituitary gland may cause testosterone or other hormone deficiencies.
Also, treatment for a brain tumor, such as surgery or radiation therapy, can affect the pituitary gland and cause hypogonadism.
- Inflammatory disease. Certain inflammatory diseases, such as sarcoidosis, histiocytosis and tuberculosis, involve the hypothalamus and pituitary gland and can affect testosterone production.
- HIV/AIDS. HIV/AIDS can cause low levels of testosterone by affecting the hypothalamus, the pituitary and the testes.
- Medications. The use of certain drugs, such as opiate pain medications and some hormones, can affect testosterone production.
- Obesity. Being significantly overweight at any age might be linked to hypogonadism.
- Aging. As men age, there’s a slow, progressive decrease in testosterone production. The rate varies greatly.
Risk factors for hypogonadism include:
- Human immunodeficiency virus (HIV) / Acquired immunodeficiency syndrome (AIDS)
- Previous chemotherapy or radiation therapy
- Aging
- Obesity
- Malnutrition
Hypogonadism can be inherited. If any of these risk factors are in your family health history, tell your doctor.
Complications
The complications of untreated hypogonadism differ depending on when it develops — during fetal development, puberty or adulthood.
Complications might include:
- Abnormal genitalia
- Enlarged male breasts (gynecomastia)
- Infertility
- Erectile dysfunction
- Osteoporosis
- Poor self-image
Diagnosis
Early detection in boys can help prevent problems from delayed puberty. Early diagnosis and treatment in men offer better protection against osteoporosis and other related conditions.
Your health care provider will conduct a physical exam and note whether your sexual development, such as your pubic hair, muscle mass and size of your testes, is consistent with your age.
Your provider will test your blood level of testosterone if you have signs or symptoms of hypogonadism. Because testosterone levels vary and are generally highest in the morning, blood testing is usually done early in the day, before 10 a.m., possibly on more than one day.
If tests confirm that you have low testosterone, further testing can determine if a testicular disorder or a pituitary abnormality is the cause. These studies might include:
- Hormone testing
- Semen analysis
- Pituitary imaging
- Genetic studies
- Testicular biopsy
Treatment
Adults
Testosterone replacement can raise testosterone levels and help ease the symptoms of male hypogonadism. These include less desire for sex, less energy, less facial and body hair, and loss of muscle mass and bone mass.
For older adults who have low testosterone and symptoms of hypogonadism due to aging, it’s less clear how well testosterone replacement works.
Anyone taking testosterone replacement should have a medical checkup and blood tests several times during the first year of treatment and yearly after that. This is to see how well the treatment works and to watch for side effects.
Types of testosterone replacement therapy
Testosterone taken by mouth, also called oral, isn’t often used for treatment of hypogonadism. Oral testosterone can cause serious liver problems. And it doesn’t keep testosterone levels even.
The U.S. Food and Drug Administration has approved one oral testosterone replacement, testosterone undecanoate (Jatenzo, Tlando, Kyzatrex). The lymph system absorbs it, so it might not cause the liver problems seen with other oral forms of testosterone. It’s not used to treat hypogonadism caused by aging.
Other forms you might choose can depend on how easy they are to get and use, how much they cost, and whether insurance covers them. They include:
-
Gels. There are several available with different ways of applying them. Depending on the brand, you rub the testosterone into your skin on your upper arm or shoulder (AndroGel, Testim, Vogelxo) or apply it to the front and inner thigh (Fortesta).
The body soaks in testosterone through the skin. Don’t shower or bathe for several hours after a using a gel to give it time to soak in.
Side effects include skin irritation and, if someone touches you, having the medicine get on someone else. Don’t let your skin touch anyone until the gel is fully dry. Or cover the area after putting on the gel.
-
Shot. Testosterone cypionate (Depo-Testosterone) and testosterone enanthate (Xyosted) are given in a muscle or under the skin. Symptoms might vary between doses depending on how often you get the shots.
You or a family member can learn to give testosterone shots at home. If you’re not OK with giving yourself shots, a member of your care team can do it for you.
The shot form of testosterone undecanoate (Aveed) goes deep into a muscle, typically every 10 weeks. A member of your medical team must give it. It can have serious side effects.
- Patch. A patch containing testosterone is put on an arm or the torso each night. Possible side effects are mild or severe skin problems.
-
Gum and cheek, also called buccal cavity. Small and puttylike, gum-and-cheek testosterone replacement sends testosterone through the area above the top teeth where the gum meets the upper lip, called the buccal cavity.
This product, taken three times a day, sticks to the gumline and sends testosterone into the bloodstream. It can irritate the gum.
- Nasal. This testosterone gel (Natesto) can be pumped into the nostrils. This option reduces the risk that medicine will get on someone else through skin contact. This type of testosterone is put into each nostril three times a day. This might make it less easy to use than other methods.
- Pellets put under the skin, called Implants. Testosterone-containing pellets (Testopel) are surgically put under the skin every 3 to 6 months.
Testosterone therapy carries risks, including:
- Making too many red blood cells.
- Acne.
- Bigger breasts.
- Sleep problems.
- Growth of the prostate.
- Not making as much sperm.
Risks from testosterone therapy are most often due to doses that are too high. Many of these side effects go away when the dose is lowered. That’s why it’s so important to have regular follow-up visits with a health care professional, who will monitor the testosterone levels in your blood.
Treatment of infertility due to hypogonadism
If a pituitary problem is the cause, pituitary hormones can be given to help the body make more sperm and restore fertility. A pituitary tumor may need treatment with surgery, medicine, radiation or replacement of other hormones.
There’s often no way to help men with primary hypogonadism make sperm. But there are ways to help couples who haven’t been able to have children. Assisted reproductive technology offers ways to help.
Treatment for boys
Treatment of delayed puberty in boys depends on the cause. Three to six months of testosterone shots can help start puberty. The testosterone can help increase muscle mass, beard and pubic hair growth, and growth of the penis. This treatment is given only if the bones have matured enough.
Coping and support
Having male hypogonadism can affect your self-image and, possibly, your relationships. Talk with your health care provider about how you can reduce the anxiety and stress that often accompany these conditions. Many men benefit from psychological or family counseling.
Find out if there are support groups in your area or online. Support groups put you in touch with other people with similar challenges.
Preparing for your appointment
Although you’re likely to start by seeing your family doctor or other care provider, you might be referred to someone who specializes in the hormone-producing glands (endocrinologist).
Here’s some information to help you get ready for your appointment.
What you can do
Make a list of:
- Your symptoms, including any that may seem unrelated to the reason for which you scheduled the appointment, and when they began
- Key personal information, including any major stresses, recent life changes, and history of childhood illnesses or surgeries
- All medications, vitamins or other supplements you take, including doses
- Questions to ask your provider
For male hypogonadism, some questions to ask your provider include:
- What’s the most likely cause of my symptoms?
- Are there other possible causes for my symptoms?
- What tests do I need?
- Is my condition likely temporary or chronic?
- What treatments are available?
- I have other health conditions. How can I best manage them together?
- Are there restrictions I need to follow?
- Are there brochures or other printed material I can have? What websites do you recommend?
Don’t hesitate to ask other questions.
What to expect from your provider
Be prepared to answer questions about your condition, such as:
- Have your symptoms been continuous or occasional?
- How severe are your symptoms?
- What, if anything, seems to improve your symptoms?
- What, if anything, appears to worsen your symptoms?
- When did you begin puberty? Did it seem to be earlier or later than your peers?
- Did you have any growth problems as a child or adolescent?
- Have you injured your testicles?
- Did you have the mumps as a child or teen? Do you recall if you felt pain in your testicles while you had the mumps?
- Did you have undescended testicles as a baby?
- Did you have surgery for a groin hernia or genital surgery as a child?
© 1998-2025 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use

