

Heavy menstrual bleeding
![]() November, 20th, 2024
November, 20th, 2024
Benefit Summary
Learn about the causes and treatment of heavy menstrual periods.
Overview
, Overview, ,
Some women have menstrual bleeding that is heavy or lasts for more than a few days. This condition used to be called menorrhagia. Heavy menstrual bleeding is a common concern. But most women don’t have enough blood loss for it to be called heavy menstrual bleeding.
Some women have menstrual bleeding between periods, or earlier or later in their cycles than expected. This type of bleeding is called abnormal uterine bleeding or irregular menstrual bleeding.
With heavy menstrual bleeding, blood flow and cramping make it harder to do your usual activities. If you dread your period because you have heavy menstrual bleeding, talk with your doctor. There are many treatments that can help.
Symptoms
Symptoms of heavy menstrual bleeding may include:
- Soaking through one or more sanitary pads or tampons every hour for several hours in a row.
- Needing double sanitary protection to control your menstrual flow.
- Getting up at night to change sanitary pads or tampons.
- Bleeding for more than a week.
- Passing blood clots larger than a quarter.
- Limiting daily activities due to heavy menstrual flow.
- Feeling tired, fatigued or short of breath as the result of blood loss.
When to see a doctor
Seek medical help before your next scheduled exam if you have:
- Vaginal bleeding so heavy it soaks at least one pad or tampon an hour for more than two hours in a row.
- Bleeding between periods or unusual vaginal bleeding.
- Vaginal bleeding after menopause.
Causes
In some cases, the reason for heavy menstrual bleeding is unknown. But a number of conditions may cause heavy menstrual bleeding. They include:
-
Hormones being out of balance. In a typical menstrual cycle, there’s a balance between the hormones estrogen and progesterone. This controls the buildup of the lining of the uterus. The lining of the uterus also is known as the endometrium. This lining is shed during a menstrual period. When hormones are out of balance, the lining becomes too thick and sheds by way of heavy menstrual bleeding or unexpected bleeding between periods.
A number of conditions can cause hormone imbalances. These include obesity, insulin resistance, thyroid problems and polycystic ovary syndrome, which also is called PCOS.
- Problems with the ovaries. Sometimes ovaries don’t release an egg during a menstrual cycle. This also is known as anovulation. When this happens, the body doesn’t make the hormone progesterone the way it usually does during a menstrual cycle. This leads to hormone imbalance and may result in heavy menstrual bleeding or unexpected bleeding between periods.
- Uterine fibroids. These tumors develop during childbearing years. They are benign, which means they are not cancerous. Uterine fibroids may cause heavier than normal menstrual bleeding or bleeding that goes on for a long time.
- Polyps. These small growths on the lining of the uterus may cause menstrual bleeding that is heavy or lasts for a long time. They may cause bleeding between periods. Polyps also can cause spotting or bleeding after menopause. The growths are not cancerous.
- Adenomyosis. In this condition, glands from the lining of the uterus grow into the wall of the uterus itself. This can cause heavy bleeding and painful periods.
- Intrauterine device, also called an IUD. Heavy menstrual bleeding is a well-known side effect of using a hormone-free IUD for birth control. Talk to your doctor about other birth control options. IUDs with progestin may ease heavy menstrual bleeding.
- Pregnancy complications. A single, heavy, late period may be due to a miscarriage. Another cause of heavy bleeding during pregnancy includes the unusual location of the placenta, which supplies nutrition to the baby and removes waste. The placenta may be too low or covering the opening of the uterus, which is called the cervix. This condition also is known as placenta previa.
- Cancer. Cancer of the uterus or cervix can cause abnormal uterine bleeding, unexpected or heavy menstrual bleeding. These cancers can happen before or after menopause. Women who have had an abnormal Pap test in the past are at higher risk of cervical cancer.
- Genetic bleeding disorders. Some bleeding disorders that run in families cause heavy menstrual bleeding. These include von Willebrand’s disease, a condition in which the blood does not clot properly.
- Medicines. Some medicines can result in heavy or lengthy menstrual bleeding. These include hormonal medicines such as birth control pills that have estrogen and progestin. These medicines typically help lessen menstrual bleeding but sometimes cause unexpected bleeding between periods. Medicines that prevent blood clots also may cause heavy menstrual bleeding. They include warfarin (Jantoven), enoxaparin (Lovenox), apixaban (Eliquis) and rivaroxaban (Xarelto).
- Other medical conditions. A number of other medical conditions may cause heavy menstrual bleeding. They include liver, kidney and thyroid disease.
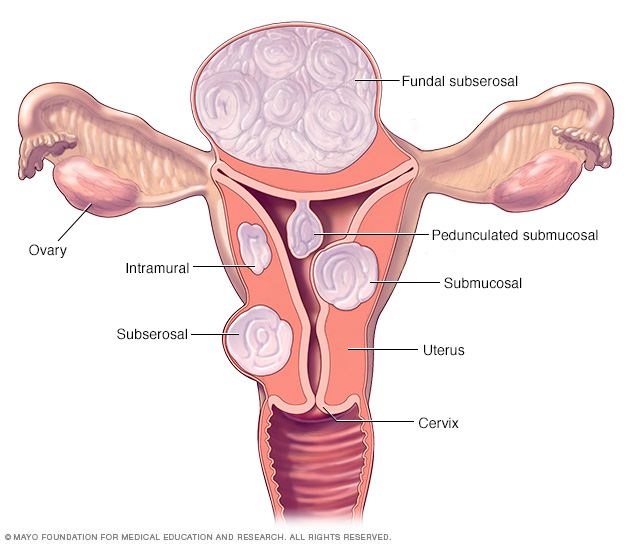
There are three major types of uterine fibroids. Intramural fibroids grow within the muscular uterine wall. Submucosal fibroids bulge into the uterine cavity. Subserosal fibroids project to the outside of the uterus. Some submucosal or subserosal fibroids may be pedunculated. This means they hang from a stalk inside or outside the uterus.

Uterine polyps attach to the uterus by a large base or a thin stalk. They can grow to be several centimeters in size. Uterine polyps can cause irregular menstrual bleeding, bleeding after menopause, very heavy menstrual flow or bleeding between periods.

With adenomyosis, the same type of tissue that lines the uterus is present within the muscles that make up the walls of the uterus. It also can grow from the surface of the uterus into the walls of the uterus. This tissue also is known as endometrial tissue.
Adenomyosis Risk factors
Risk factors vary with age and the medical conditions you have. Usually, the release of an egg from the ovaries signals the body to make progesterone. Progesterone is the hormone most responsible for keeping periods regular. If no egg is released, the body does not make enough progesterone. This can result in heavy menstrual bleeding or unexpected bleeding between periods.
In teenagers, an irregular period or heavy menstrual bleeding often happens when an egg is not released during a monthly cycle. Teenagers are most likely to have cycles without an egg release during the first year after they have their first period.
In older women of reproductive age, heavy menstrual bleeding is often caused by problems with the uterus. These include fibroids, polyps and adenomyosis. But other problems also could cause heavy menstrual bleeding. Examples include cancer of the uterus, bleeding disorders, side effects of medicines, and liver or kidney disease.
Complications
Menstrual bleeding that is too heavy or lasts too long can lead to other medical conditions. These include:
-
Anemia. Heavy menstrual bleeding can cause anemia related to blood loss. Anemia is a condition in which the body lacks enough red blood cells to carry oxygen to tissues. The number of red blood cells is measured by hemoglobin. Hemoglobin is a protein in red blood cells that carries oxygen to tissues throughout the body.
Iron deficiency anemia occurs as the body tries to make up for lost red blood cells. The body uses iron stores to make more hemoglobin so that enough oxygen can be carried to tissues. Heavy menstrual bleeding may make iron levels too low. This may result in iron deficiency anemia.
Symptoms include headaches and feeling tired. Although diet plays a role in iron deficiency anemia, the problem is made worse by heavy menstrual periods.
- Severe pain. Along with heavy menstrual bleeding, you might have painful menstrual cramps. This also is known as dysmenorrhea. Talk to your doctor if your cramps make it hard to do your daily activities.
Diagnosis
A member of your health care team will likely ask about your medical history and menstrual cycles. You may be asked to keep a diary to track days with and without bleeding. Record information such as how heavy your flow was and how many sanitary pads or tampons you needed to control it.
After doing a physical exam, your doctor or other member of your care team may recommend certain tests or procedures. They may include:
- Blood tests. A sample of your blood may be tested for iron deficiency anemia. The sample also may be tested for other conditions, such as thyroid disorders or blood-clotting problems.
- Pap test. In this test, cells from your cervix are collected. They are tested for inflammation or changes that may be precancerous, which means they could lead to cancer. Cells also are tested for human papilloma virus in women ages 25 to 30 and older.
- Endometrial biopsy. Your doctor may take a tissue sample from the inside of your uterus. A pathologist will look for signs of cancer or precancer of the uterus.
- Ultrasound. This imaging method uses sound waves to create pictures of your uterus, ovaries and pelvis.
Results of these initial tests may lead to more testing, including:
- Sonohysterography. During this test, a fluid is injected through a tube into your uterus by way of your vagina and cervix. Your doctor then uses ultrasound to look for problems in the lining of your uterus.
- Hysteroscopy. A thin, lighted instrument is inserted through your vagina and cervix into your uterus. This allows your doctor to see the inside of your uterus.
Your doctor can make a diagnosis of heavy menstrual bleeding or abnormal uterine bleeding only after it’s known that something else isn’t causing your condition. These causes may include menstrual disorders, medical conditions or medicines.

During hysterosonography (his-tur-o-suh-NOG-ruh-fee), you have a thin, flexible tube called a catheter placed in the uterus. Salt water, also called saline, is injected through the flexible tube into the hollow part of the uterus. An ultrasound probe transmits images of the inside of the uterus to a nearby monitor.

During hysteroscopy (his-tur-OS-kuh-pee), a thin, lighted instrument provides a view of the inside of the uterus. This instrument also is called a hysteroscope.
Hysteroscopy Treatment
Treatment for heavy menstrual bleeding is based on a number of factors. These include:
- Your overall health and medical history.
- The cause of the condition and how serious it is.
- How well you tolerate certain medicines or procedures.
- The chance that your periods will soon become less heavy.
- Your plans to have children.
- How the condition affects your lifestyle.
- Your opinion or personal choices.
Medicines
Medicines for heavy menstrual bleeding may include:
- Nonsteroidal anti-inflammatory drugs, also called NSAIDs. NSAIDs, such as ibuprofen (Advil, Motrin IB, others) or naproxen sodium (Aleve), help reduce menstrual blood loss. NSAIDs may also make menstrual cramps less painful.
- Tranexamic acid. Tranexamic acid (Lysteda) helps reduce menstrual blood loss. This medicine only needs to be taken at the time of bleeding.
- Oral contraceptives. Aside from birth control, oral contraceptives can help regulate menstrual cycles and ease menstrual bleeding that is heavy or lasts a long time.
- Oral progesterone. The natural hormone progesterone can help fix hormone imbalance and reduce heavy menstrual bleeding. The synthetic form of progesterone is called progestin.
- Hormonal IUD (Mirena, Liletta, others). This intrauterine device releases a type of progestin called levonorgestrel. It makes the uterine lining thin and reduces menstrual blood flow and cramping.
- Other medicines. Gonadotropin-releasing hormone agonists and antagonists are also called GnRH medicines. They help control heavy uterine bleeding. Relugolix combined with an estrogen and progestin (Myfembree) may help control bleeding caused by fibroids. Elagolix with an estrogen and progestin (Oriahnn) is used to treat fibroid-related bleeding. Elagolix alone (Orilissa) may help control bleeding caused by endometriosis.
If you have heavy menstrual bleeding from taking hormone medicine, you may need to stop or change your medicine.
If you have anemia due to heavy menstrual bleeding, you may need to take iron supplements. If your iron levels are low but you’re not yet anemic, you may be started on iron supplements instead of waiting until you become anemic.
Procedures
You may need surgery for heavy menstrual bleeding if medicines do not help. Treatment options include:
- Dilation and curettage, also called a D&C. In this procedure, your doctor opens your cervix. This also is called dilating the cervix. The doctor then scrapes or suctions tissue from the lining of your uterus. This also is known as curettage. You may have a D&C to find the source of abnormal uterine bleeding. Causes of bleeding may include polyps, fibroids or cancer of the uterus. If you’ve had a miscarriage, you may need a D&C to completely empty the uterus. Hysteroscopy is often used with D&C to help doctors find the source of bleeding in the uterus.
- Uterine artery embolization. The goal of this procedure is to block blood flow to uterine fibroids. Blocking blood flow to fibroids helps to shrink them. During the procedure, the surgeon passes a catheter through the large artery in the thigh. This also is known as the femoral artery. The surgeon guides the catheter to the blood vessels in the uterus and injects tiny beads or sponges to reduce blood flow to the fibroid.
- Focused ultrasound. This procedure shrinks fibroids by targeting and destroying fibroids through ultrasound waves and radiofrequency energy. It needs no incisions.
- Myomectomy. This is the surgical removal of uterine fibroids. Depending on the size, number and location of the fibroids, your surgeon may perform the myomectomy through several small incisions in the abdomen. This is known also as the laparoscopic approach. Or the surgeon may put a thin, flexible tube into the vagina and cervix to see and remove fibroids or polyps inside the uterus. This also is called the hysteroscopic approach.
-
Endometrial ablation. This procedure involves destroying the lining of the uterus. The process of destroying tissue also is known as ablation. The surgeon uses a laser, radio waves or heat applied to the lining of the uterus to destroy the tissue.
After endometrial ablation, you may have much lighter periods. Pregnancy after endometrial ablation isn’t likely but is possible and could be dangerous. Using reliable or permanent birth control until menopause is recommended.
- Endometrial resection. The surgeon uses an electrosurgical wire loop to remove the lining of the uterus. Pregnancy isn’t recommended after this procedure.
- Hysterectomy. In this procedure, the uterus and cervix are removed. It ends menstrual periods and the ability to get pregnant. Hysterectomy is performed under anesthesia and may require a short hospital stay. Early menopause may occur if the ovaries are removed. The procedure to remove both ovaries is called bilateral oophorectomy.
Many of these surgical procedures are done on an outpatient basis. You may need a general anesthetic but it’s likely that you can go home on the same day. With an abdominal myomectomy or a hysterectomy, you may need a brief hospital stay.
Sometimes heavy menstrual bleeding is a sign of another condition, such as thyroid disease. In those cases, treating the condition usually results in lighter periods.
Preparing for an appointment
You may start by seeing your primary care doctor or other health care professional. Or you may be referred immediately to a specialist called an obstetrician/gynecologist.
Here’s some information to help you get ready for your appointment.
What you can do
When you make the appointment, ask if there’s anything you need to do in advance, such as fasting before having a specific test. Make a list of:
- Your symptoms, including any that seem unrelated to the reason for your appointment.
- Key personal information, including major stresses, recent life changes and family medical history.
- All medications, vitamins or supplements you take, including the doses.
- Questions to ask your doctor.
Take a family member or friend along, if possible, to help you remember the information you’re given.
For heavy menstrual bleeding, some basic questions to ask your care team include:
- What’s likely causing my symptoms?
- Other than the most likely cause, what are other possible causes for my symptoms?
- What tests do I need?
- Is my condition likely temporary or will it be ongoing?
- What are my treatment options?
- I have these other health conditions. How can I best manage them together?
- Should I see a specialist?
- Are there brochures or other printed material I can have? What websites do you recommend?
Don’t hesitate to ask any other questions as they occur to you during your appointment.
What to expect from your doctor
You may be asked certain questions during your appointment, such as:
- When did your symptoms begin?
- Have your symptoms been continuous or occasional?
- How severe are your symptoms?
- What, if anything, seems to improve your symptoms?
- What, if anything, seems to worsen your symptoms?
What you can do in the meantime
Avoid doing anything that seems to worsen your symptoms.
© 1998-2025 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use

