

Diabetic retinopathy
![]() August, 10th, 2023
August, 10th, 2023
Benefit Summary
Good diabetes control and regular exams can help prevent this diabetes complication that affects the eyes. Find out how.
Overview
, Overview, ,
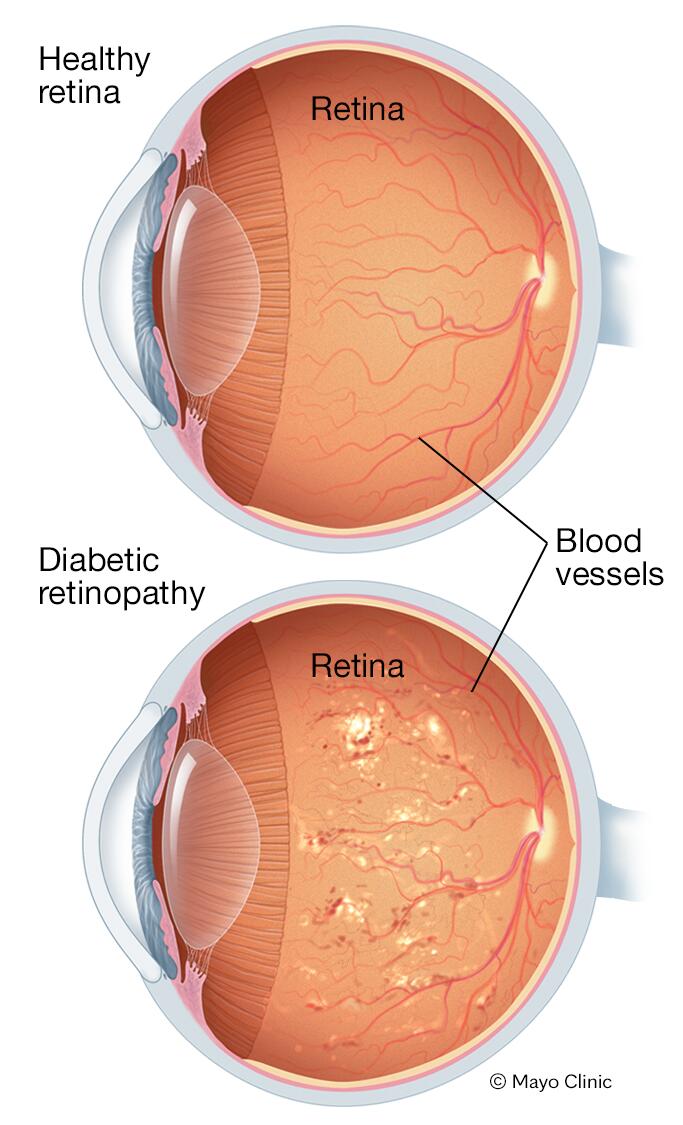
Diabetic retinopathy (die-uh-BET-ik ret-ih-NOP-uh-thee) is a diabetes complication that affects eyes. It’s caused by damage to the blood vessels of the light-sensitive tissue at the back of the eye (retina).
At first, diabetic retinopathy might cause no symptoms or only mild vision problems. But it can lead to blindness.
The condition can develop in anyone who has type 1 or type 2 diabetes. The longer you have diabetes and the less controlled your blood sugar is, the more likely you are to develop this eye complication.
Symptoms
You might not have symptoms in the early stages of diabetic retinopathy. As the condition progresses, you might develop:
- Spots or dark strings floating in your vision (floaters)
- Blurred vision
- Fluctuating vision
- Dark or empty areas in your vision
- Vision loss
When to see an eye doctor
Careful management of your diabetes is the best way to prevent vision loss. If you have diabetes, see your eye doctor for a yearly eye exam with dilation — even if your vision seems fine.
Developing diabetes when pregnant (gestational diabetes) or having diabetes before becoming pregnant can increase your risk of diabetic retinopathy. If you’re pregnant, your eye doctor might recommend additional eye exams throughout your pregnancy.
Contact your eye doctor right away if your vision changes suddenly or becomes blurry, spotty or hazy.
Causes
Over time, too much sugar in your blood can lead to the blockage of the tiny blood vessels that nourish the retina, cutting off its blood supply. As a result, the eye attempts to grow new blood vessels. But these new blood vessels don’t develop properly and can leak easily.
There are two types of diabetic retinopathy:
-
Early diabetic retinopathy. In this more common form — called nonproliferative diabetic retinopathy (NPDR) — new blood vessels aren’t growing (proliferating).
When you have NPDR, the walls of the blood vessels in your retina weaken. Tiny bulges protrude from the walls of the smaller vessels, sometimes leaking fluid and blood into the retina. Larger retinal vessels can begin to dilate and become irregular in diameter as well. NPDR can progress from mild to severe as more blood vessels become blocked.
Sometimes retinal blood vessel damage leads to a buildup of fluid (edema) in the center portion (macula) of the retina. If macular edema decreases vision, treatment is required to prevent permanent vision loss.
-
Advanced diabetic retinopathy. Diabetic retinopathy can progress to this more severe type, known as proliferative diabetic retinopathy. In this type, damaged blood vessels close off, causing the growth of new, abnormal blood vessels in the retina. These new blood vessels are fragile and can leak into the clear, jellylike substance that fills the center of your eye (vitreous).
Eventually, scar tissue from the growth of new blood vessels can cause the retina to detach from the back of your eye. If the new blood vessels interfere with the normal flow of fluid out of the eye, pressure can build in the eyeball. This buildup can damage the nerve that carries images from your eye to your brain (optic nerve), resulting in glaucoma.
Anyone who has diabetes can develop diabetic retinopathy. The risk of developing the eye condition can increase as a result of:
- Having diabetes for a long time
- Poor control of your blood sugar level
- High blood pressure
- High cholesterol
- Pregnancy
- Tobacco use
- Being Black, Hispanic or Native American
Complications
Diabetic retinopathy involves the growth of abnormal blood vessels in the retina. Complications can lead to serious vision problems:
-
Vitreous hemorrhage. The new blood vessels may bleed into the clear, jellylike substance that fills the center of your eye. If the amount of bleeding is small, you might see only a few dark spots (floaters). In more-severe cases, blood can fill the vitreous cavity and completely block your vision.
Vitreous hemorrhage by itself usually doesn’t cause permanent vision loss. The blood often clears from the eye within a few weeks or months. Unless your retina is damaged, your vision will likely return to its previous clarity.
- Retinal detachment. The abnormal blood vessels associated with diabetic retinopathy stimulate the growth of scar tissue, which can pull the retina away from the back of the eye. This can cause spots floating in your vision, flashes of light or severe vision loss.
- Glaucoma. New blood vessels can grow in the front part of your eye (iris) and interfere with the normal flow of fluid out of the eye, causing pressure in the eye to build. This pressure can damage the nerve that carries images from your eye to your brain (optic nerve).
- Blindness. Diabetic retinopathy, macular edema, glaucoma or a combination of these conditions can lead to complete vision loss, especially if the conditions are poorly managed.
Prevention
You can’t always prevent diabetic retinopathy. However, regular eye exams, good control of your blood sugar and blood pressure, and early intervention for vision problems can help prevent severe vision loss.
If you have diabetes, reduce your risk of getting diabetic retinopathy by doing the following:
- Manage your diabetes. Make healthy eating and physical activity part of your daily routine. Try to get at least 150 minutes of moderate aerobic activity, such as walking, each week. Take oral diabetes medications or insulin as directed.
- Monitor your blood sugar level. You might need to check and record your blood sugar level several times a day — or more frequently if you’re ill or under stress. Ask your doctor how often you need to test your blood sugar.
- Ask your doctor about a glycosylated hemoglobin test. The glycosylated hemoglobin test, or hemoglobin A1C test, reflects your average blood sugar level for the two- to three-month period before the test. For most people with diabetes, the A1C goal is to be under 7%.
- Keep your blood pressure and cholesterol under control. Eating healthy foods, exercising regularly and losing excess weight can help. Sometimes medication is needed, too.
- If you smoke or use other types of tobacco, ask your doctor to help you quit. Smoking increases your risk of various diabetes complications, including diabetic retinopathy.
- Pay attention to vision changes. Contact your eye doctor right away if your vision suddenly changes or becomes blurry, spotty or hazy.
Remember, diabetes doesn’t necessarily lead to vision loss. Taking an active role in diabetes management can go a long way toward preventing complications.
Diagnosis
Diabetic retinopathy is best diagnosed with a comprehensive dilated eye exam. For this exam, drops placed in your eyes widen (dilate) your pupils to allow your doctor a better view inside your eyes. The drops can cause your close vision to blur until they wear off, several hours later.
During the exam, your eye doctor will look for abnormalities in the inside and outside parts of your eyes.
- Fluorescein angiography
-
After your eyes are dilated, a dye is injected into a vein in your arm. Then pictures are taken as the dye circulates through your eyes’ blood vessels. The images can pinpoint blood vessels that are closed, broken or leaking.
- Optical coherence tomography (OCT)
-
With this test, pictures provide cross-sectional images of the retina that show the thickness of the retina. This will help determine how much fluid, if any, has leaked into retinal tissue. Later, OCT exams can be used to monitor how treatment is working.
Treatment
Treatment, which depends largely on the type of diabetic retinopathy you have and how severe it is, is geared to slowing or stopping the progression.
- Early diabetic retinopathy
-
If you have mild or moderate nonproliferative diabetic retinopathy, you might not need treatment right away. However, your eye doctor will closely monitor your eyes to determine when you might need treatment.
Work with your diabetes doctor (endocrinologist) to determine if there are ways to improve your diabetes management. When diabetic retinopathy is mild or moderate, good blood sugar control can usually slow the progression.
- Advanced diabetic retinopathy
-
If you have proliferative diabetic retinopathy or macular edema, you’ll need prompt treatment. Depending on the specific problems with your retina, options might include:
-
Injecting medications into the eye. These medications, called vascular endothelial growth factor inhibitors, are injected into the vitreous of the eye. They help stop growth of new blood vessels and decrease fluid buildup.
Three drugs are approved by the U.S. Food and Drug Administration (FDA) for treatment of diabetic macular edema — faricimab-svoa (Vabysmo), ranibizumab (Lucentis) and aflibercept (Eylea). A fourth drug, bevacizumab (Avastin), can be used off-label for the treatment of diabetic macular edema.
These drugs are injected using topical anesthesia. The injections can cause mild discomfort, such as burning, tearing or pain, for 24 hours after the injection. Possible side effects include a buildup of pressure in the eye and infection.
These injections will need to be repeated. In some cases, the medication is used with photocoagulation.
-
Photocoagulation. This laser treatment, also known as focal laser treatment, can stop or slow the leakage of blood and fluid in the eye. During the procedure, leaks from abnormal blood vessels are treated with laser burns.
Focal laser treatment is usually done in your doctor’s office or eye clinic in a single session. If you had blurred vision from macular edema before surgery, the treatment might not return your vision to normal, but it’s likely to reduce the chance of the macular edema worsening.
-
Panretinal photocoagulation. This laser treatment, also known as scatter laser treatment, can shrink the abnormal blood vessels. During the procedure, the areas of the retina away from the macula are treated with scattered laser burns. The burns cause the abnormal new blood vessels to shrink and scar.
It’s usually done in your doctor’s office or eye clinic in two or more sessions. Your vision will be blurry for about a day after the procedure. Some loss of peripheral vision or night vision after the procedure is possible.
- Vitrectomy. This procedure uses a tiny incision in your eye to remove blood from the middle of the eye (vitreous) as well as scar tissue that’s tugging on the retina. It’s done in a surgery center or hospital using local or general anesthesia.
-
While treatment can slow or stop the progression of diabetic retinopathy, it’s not a cure. Because diabetes is a lifelong condition, future retinal damage and vision loss are still possible.
Even after treatment for diabetic retinopathy, you’ll need regular eye exams. At some point, you might need additional treatment.
Alternative medicine
Several alternative therapies have suggested some benefits for people with diabetic retinopathy, but more research is needed to understand whether these treatments are effective and safe.
Let your doctor know if you take herbs or supplements. They can interact with other medications or cause complications in surgery, such as excessive bleeding.
It’s vital not to delay standard treatments to try unproven therapies. Early treatment is the best way to prevent vision loss.
Coping and support
The thought that you might lose your sight can be frightening, and you may benefit from talking to a therapist or finding a support group. Ask your doctor for referrals.
If you’ve already lost vision, ask your doctor about low-vision products, such as magnifiers, and services that can make daily living easier.
Preparing for your appointment
The American Diabetes Association (ADA) recommends that people with type 1 diabetes have an eye exam within five years of being diagnosed. If you have type 2 diabetes, the ADA advises getting your initial eye exam at the time of your diagnosis.
If there’s no evidence of retinopathy on your initial exam, the ADA recommends that people with diabetes get dilated and comprehensive eye exams at least every two years. If you have any level of retinopathy, you’ll need eye exams at least annually. Ask your eye doctor what he or she recommends.
The ADA recommends that women with diabetes have an eye exam before becoming pregnant or during the first trimester of pregnancy and be closely followed during the pregnancy and up to one year after giving birth. Pregnancy can sometimes cause diabetic retinopathy to develop or worsen.
Here’s some information to help you get ready for your eye appointment.
What you can do
- Write a brief summary of your diabetes history, including when you were diagnosed; medications you have taken for diabetes, now and in the past; recent average blood sugar levels; and your last few hemoglobin A1C readings, if you know them.
- List all medications, vitamins and other supplements you take, including dosages.
- List your symptoms, if any. Include those that may seem unrelated to your eyes.
- Ask a family member or friend to go with you, if possible. Someone who accompanies you can help remember the information you receive. Also, because your eyes will be dilated, a companion can drive you home.
- List questions for your doctor.
For diabetic retinopathy, questions to ask your doctor include:
- How is diabetes affecting my vision?
- Do I need other tests?
- Is this condition temporary or long lasting?
- What treatments are available, and which do you recommend?
- What side effects might I expect from treatment?
- I have other health conditions. How can I best manage them together?
- If I control my blood sugar, will my eye symptoms improve?
- What do my blood sugar goals need to be to protect my eyes?
- Can you recommend services for people with visual impairment?
Don’t hesitate to ask other questions you have.
What to expect from your doctor
Your doctor is likely to ask you questions, including:
- Do you have eye symptoms, such as blurred vision or floaters?
- How long have you had symptoms?
- In general, how well are you controlling your diabetes?
- What was your last hemoglobin A1C?
- Do you have other health conditions, such as high blood pressure or high cholesterol?
- Have you had eye surgery?
