

Radiation therapy for breast cancer
![]() January, 10th, 2025
January, 10th, 2025
Summary
Find out why doctors use radiation treat breast cancer. Learn what to expect and the side effects of breast cancer radiation, including proton therapy.
Overview
, Overview, ,
Radiation therapy for breast cancer uses high-energy X-rays, protons or other particles to kill cancer cells. Rapidly growing cells, such as cancer cells, are more susceptible to the effects of radiation therapy than are normal cells.
The X-rays or particles are painless and invisible. You are not radioactive after treatment, so it is safe to be around other people, including children.
Radiation therapy for breast cancer may be delivered through:
- External radiation. A machine delivers radiation from outside your body to the breast. This is the most common type of radiation therapy used for breast cancer.
- Internal radiation (brachytherapy). After you have surgery to remove the cancer, your doctor temporarily places a radiation-delivery device in your breast in the area where the cancer once was. A radioactive source is placed into the device for short periods of time over the course of your treatment.
Radiation therapy may be used to treat breast cancer at almost every stage. Radiation therapy is an effective way to reduce your risk of breast cancer recurring after surgery. In addition, it is commonly used to ease the symptoms caused by cancer that has spread to other parts of the body (metastatic breast cancer).
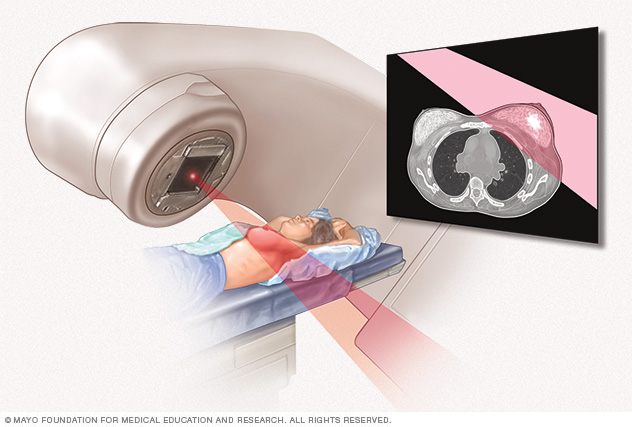
External beam radiation uses high-powered beams of energy to kill cancer cells. Beams of radiation are precisely aimed at the cancer using a machine that moves around your body.
Radiation therapy Why it’s done
Radiation therapy kills cancer cells. It’s often used after surgery to reduce the risk that the cancer will come back. It can also be used to provide relief from pain and other symptoms of advanced breast cancer.
Radiation after lumpectomy
If you’re having an operation to remove the breast cancer and leave the remaining breast tissue intact (lumpectomy or breast-conserving surgery), your doctor may recommend radiation after your procedure to kill any cancer cells that might remain. Adding radiation after a lumpectomy reduces the risk that cancer will return in the affected breast.
Lumpectomy combined with radiation therapy is often referred to as breast conservation therapy. This type of treatment is as effective as having all the breast tissue removed (mastectomy). In special situations where the risk of recurrence is very low, your doctor may also discuss the option of avoiding radiation after a lumpectomy.
After lumpectomy, radiation treatment options might include:
- Radiation to the entire breast. One of the most common types of radiation therapy after a lumpectomy is external beam radiation of the whole breast (whole-breast irradiation).
- Radiation to part of the breast. Radiation therapy to part of the breast (partial-breast irradiation) may be an option for some early-stage breast cancers. This technique directs internal or external radiation to the area around where the cancer was removed.
Radiation after mastectomy
Radiation can also be used after mastectomy. In this situation, the radiation can kill any cancer cells that might remain and reduce the risk that the cancer may recur in the remaining tissues of the chest wall or lymph nodes.
When determining whether you should undergo radiation after mastectomy, your doctor considers whether you have:
- Lymph nodes with signs of breast cancer. Underarm (axillary) lymph nodes that test positive for cancer cells are an indication that some cancer cells have spread beyond the breast.
- Large tumor size. A breast cancer larger than about 2 inches (5 centimeters) generally carries a higher risk of recurrence than do smaller cancers.
- Tissue margins with signs of breast cancer. After breast tissue is removed, the margins of the tissue are examined for signs of cancer cells. Very narrow margins or margins that test positive for cancer cells are a risk factor for recurrence.
Radiation for locally advanced breast cancer
Radiation therapy can also be used to treat:
- Breast cancers that can’t be removed with surgery.
- Inflammatory breast cancer, an aggressive type of cancer that spreads to the lymph channels of the skin covering the breast. This type of cancer is typically treated with chemotherapy before a mastectomy, followed by radiation, to decrease the chance of recurrence.
Radiation for managing metastatic breast cancer
If your breast cancer has spread (metastasized) to other parts of your body, radiation therapy may be recommended to shrink the cancer and help control symptoms such as pain.
Risks
Side effects from radiation therapy differ significantly depending on the type of treatment and which tissues are treated. Side effects tend to be most significant toward the end of your radiation treatment. After your sessions are complete, it may be several days or weeks before side effects clear up.
Common side effects during treatment may include:
- Mild to moderate fatigue
- Skin irritation, such as itchiness, redness, peeling or blistering, similar to what you might experience with a sunburn
- Breast swelling
Depending on which tissues are exposed, radiation therapy may cause or increase the risk of:
- Arm swelling (lymphedema) if the lymph nodes under the arm are treated
- Damage or complications leading to removal of an implant if you had breast reconstruction with an implant after mastectomy
Rarely, radiation therapy may cause or increase the risk of:
- Rib fracture or chest wall tenderness
- Inflamed lung tissue or heart damage
- Secondary cancers, such as bone or muscle cancers (sarcomas) or lung cancer
How you prepare
Before your radiation treatments, you’ll meet with your radiation therapy team, which may include:
- A radiation oncologist, a doctor who specializes in treating cancer with radiation. Your radiation oncologist determines the appropriate therapy for you, follows your progress and adjusts your treatment, if necessary.
- A radiation oncology medical physicist and a dosimetrist, who make calculations and measurements regarding your radiation dosage and its delivery.
- A radiation oncology nurse, nurse practitioner or physician assistant, who answers questions about treatments and side effects and helps you manage your health during treatment.
- Radiation therapists, who operate the radiation equipment and administer your treatments.
Before you begin treatment, your radiation oncologist will review your medical history with you and give you a physical exam to determine whether you would benefit from radiation therapy. Your doctor will also discuss the potential benefits and side effects of your radiation therapy.
Before external radiation therapy
Before your first treatment session, you’ll go through a radiation therapy planning session (simulation), in which a radiation oncologist carefully maps your breast area to target the precise location of your treatment. During the simulation:
- A radiation therapist helps you into the best position to target the affected area and avoid damage to surrounding normal tissue. Sometimes pads or other devices are used to help you hold the position.
- You have a CT scan so that the radiation oncologist can locate the treatment area and normal tissues to avoid. You’ll hear noise from the CT equipment as it moves around you. Try to relax and remain as still as possible to help ensure consistent, accurate treatments.
- A radiation therapist may mark your body with semipermanent ink or with tiny permanent tattoo dots. These marks will guide the radiation therapist in administering the radiation. Take care when washing to avoid scrubbing away the marks.
- The dosimetrist, the radiation physicist and the radiation oncologist use computer software to plan the radiation treatment you will receive. Once the simulation and planning are complete and multiple quality assurance checks are done, you can begin treatment.
Before internal radiation therapy
Before internal radiation therapy (brachytherapy) is started, a special device for placement of the radioactive material is placed in the area where the cancer was removed. This may be done during your cancer surgery or as a separate procedure several days later.
What you can expect
Radiation therapy usually begins three to eight weeks after surgery unless chemotherapy is planned. When chemotherapy is planned, radiation usually starts three to four weeks after chemotherapy is finished. You will likely have radiation therapy as an outpatient at a hospital or other treatment facility.
A common treatment schedule (course) historically has included one radiation treatment a day, five days a week (usually Monday through Friday), for five or six weeks. This course is still commonly used in people who require radiation to the lymph nodes.
Increasingly, doctors are recommending shorter treatment schedules (hypofractionated treatment). Whole-breast irradiation can frequently be shortened to one to four weeks. Partial-breast irradiation may be completed in five days or less. These hypofractionated treatment schedules work as well as the longer one and may reduce the risk of some side effects. Your radiation oncologist can help decide the course that is right for you.
During external radiation
A typical external radiation therapy session generally follows this process:
- When you arrive at the hospital or treatment facility, you’re taken to a special room that’s used specifically for radiation therapy.
- You may need to remove your clothes and put on a hospital gown.
- The radiation therapist helps you into the position you were in during the simulation process.
- The therapist may take images or X-rays to ensure that you are positioned correctly.
- The therapist leaves the room and turns on the machine that delivers the radiation (linear accelerator).
- Although the therapist isn’t in the room during the treatment, he or she will monitor you from another room on a television screen. Usually you and the therapist can talk through an intercom. If you feel sick or uncomfortable, tell your therapist, who can stop the process if necessary.
Delivery of the radiation may last only a few minutes, but expect to spend 15 to 45 minutes for each session, as it can take several minutes to set you up in the exact same position each day. This step ensures precise radiation therapy delivery.
Radiation therapy is painless. You may feel some discomfort from lying in the required position, but this is generally short-lived.
After the session, you’re free to go about your regular activities. Take any self-care steps at home that your doctor or nurse recommends, such as taking care of your skin.
In some situations, once the main radiation therapy sessions have been completed, your doctor may recommend a radiation boost. This commonly means additional fractions of radiation directed at the place of highest concern or four to five additional days of treatment. For example, after whole-breast irradiation is complete, a boost of radiation is commonly given to the area where the cancer was removed.
During internal radiation
For internal radiation, the radioactive source is inserted once or twice a day for a few minutes in the implanted radiation delivery device. This is usually done on an outpatient basis and you can leave between sessions.
After the course of treatment, the radiation delivery device is removed. You may be given pain medication before this happens. The area may be sore or tender for several days or weeks as the tissue recovers from the surgery and radiation.
Results
After you complete radiation therapy, your radiation oncologist or other medical professionals will schedule follow-up visits to monitor your progress, look for late side effects and check for signs of cancer recurrence. Make a list of questions you want to ask members of your care team.
After your radiation therapy is completed, tell your medical professional if you experience:
- Persistent pain
- New lumps, bruises, rashes or swelling
- Unexplained weight loss
- A fever or cough that doesn’t go away
- Any other bothersome symptoms
© 1998-2025 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use

